
GP information
Please follow this link for the up to date GP information: https://bomss.org/gp-hub/
10 Top Tips For GP
Management Of Patients
Post Bariatric Surgery
There is a growing cohort of people undergoing bariatric surgery, and these patients require lifelong follow-ups. Recent nice guidelines recommend
a shared care model for the long-term management of these individuals. Patients who undergo such surgery require lifelong follow up of their
comorbidities and nutritional status.
10 Top Tips to Help GP and Primary Care Staff
Tip 1: Keep a register of bariatric surgery patients. It is important to record the type of procedure in the register as the different procedures have
different risk of nutritional deficiencies.
Tip 2: Encourage patients to check their own weight and diet and to attend annual BMI and diet reviews with a health care professional
Tip 3: Symptoms of continuous vomiting, dysphagia, intestinal obstruction (gastric bypass) or severe abdominal pain requires emergency
admission under the surgical team.
Tip 4: Continue to review comorbidities post surgery, including diabetes, hypertension, hypercholesterolemia and obstructive sleep apnoea, as well
as mental health
Medication doses will need to be titrated in the post op period as weight loss occurs, but they may increase later if weight loss is not maintained.
Whether or not weight loss occurs, cardiovascular and metabolic risk factors, such as blood pressure and cholesterol levels must continue to be
monitored and treatments will need to be adjusted as required.
Mental health
There is a higher rate of mental health problems in people with severe and complex obesity compared to general population. The psychological
management of these people can be complex there should be a low threshold for referral to specialist mental health teams.
Tip 5: Review the patient’s regular medication
- The formulations may need adjustment post-surgery to allow for changes in bioavailability.
- Review comorbidity medications, such as antihypertensive, diabetes medication etc post surgery.
- Requirements are likely to fall with postoperative weight loss but may increase later if weight loss is not maintained.
- Consider pill size – patients may need liquid formulations or syrups in the immediate postoperative period. However usual medication formulations should be tolerated by around 6 weeks postoperatively.
- Replace extended-release formulations with immediate- release formulations
- Psychiatric medications may need increased or divided doses
- Use diuretic with caution due to the increased risk of hypokalaemia
- Monitor anticoagulants carefully
- Avoid non steroidal anti- inflammatory drugs if no alternative use only with a proton pump inhibitor.
- Avoid bisphosphonates
- Patients with gastric bands should avoid effervescent medication
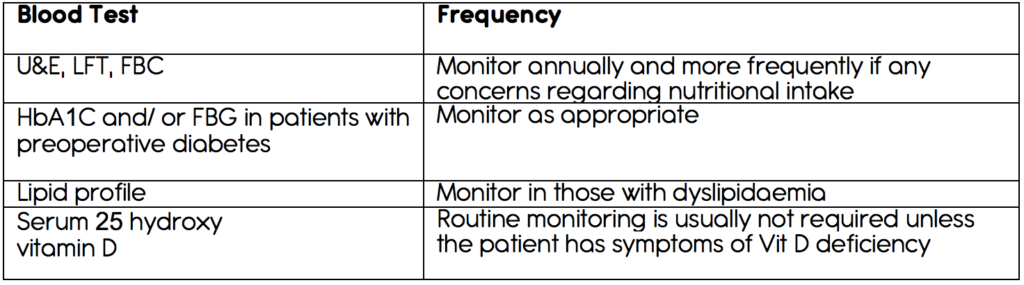
Tip 6: Bariatric surgery patients require lifelong annual blood test, including micronutrient monitoring. Encourage patients to attend their annual
blood tests.
Note patients with gastric bands require annual full blood counts, urea, and electrolyte test, liver function test, but these should be carried out earlier if there are any concerns regarding the band.
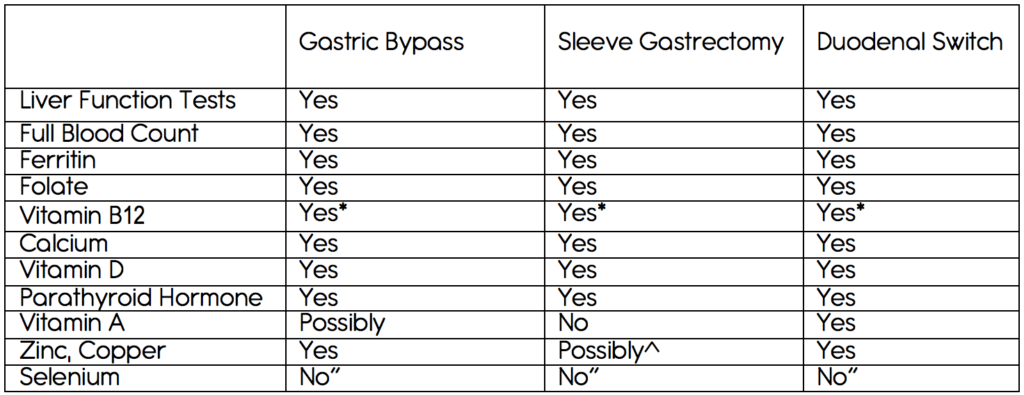
*if the patient is having 3-monthly intramuscular injections of vitamin b12, there may be no need for annual checks.
^if the patient has had a long-limb bypass or has symptoms of steatorrhoea or night blindness.
“Measure when there are deficiency concerns (see top tip seven).
Tip 7: Be aware of potential nutritional deficiencies that may occur and their signs and symptoms.
In particular, patients are at risk of anaemia and vitamin d deficiency as well as protein malnutrition and other vitamin and micronutrient
deficiencies; if a patient is deficient in one nutrient, they are likely to be deficient in others as well.
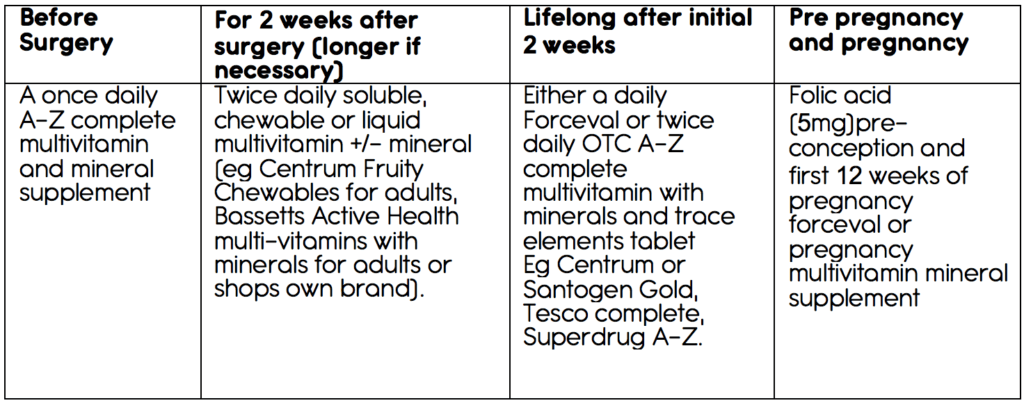
Tip 8: Ensure the patient is taking the appropriate lifelong nutritional supplements as recommended by the bariatric centre.
Tip 9: Discuss contraception – ideally, pregnancy should be avoided for at least 18-24 months post surgery.
A long acting reversible contraceptive of the patient’s choice would be appropriate. Oral contraception and the depo-provera are not
recommended because if the issue with absorption and weight gain, respectively.
Tip 10: If a patient, should plan or wish to become pregnant after bariatric surgery, alter their nutritional supplements to one suitable during
pregnancy. Pregnacare or a supplement for pregnancy support
Additional monitoring and supplementation may be required the patient should inform the bariatric team and can be reviewed by a bariatric
dietitian.
Gastric bands may need band adjustments on becoming pregnant to allow good nutritional intake and fetal growth and symptom control .